Introduction
Venous thromboembolic (VTE) disease is one of the leading causes of mortality and morbidity in developed countries. The disease can manifest itself through thrombotic obstruction of venous system and usually occurs as deep vein thrombosis of the leg. Fatal complications in the form of massive pulmonary embolism occur in 20% of cases (1).
The incidence of the VTE disease in Caucasian population has not changed during the past twenty-five years. In the white American population it occurs in 108/100,000 people a year (2). The highest incidence is in African population and the lowest in East Asia, Alaska and among the Native Americans (3–6). Venous thromboembolic disease occurs as a result of interaction related to a series of risk factors: acquired, environmental and inherited factors (7,8). The risk increases in proportion to the number of risk factors (9). Venous thromboembolic disease is highly heritable, and multiple co-inherited genetic risk factors increase the incident risk.
The most common inherited factors for thrombophilia in Caucasians are factor V (FV) R506Q (Leiden) and factor II (FII) G20210A (prothrombin) polymorphisms. The frequency of the FV Leiden in Europe varies across different geographical regions. It is the lowest in North Europe and the highest in South Europe and in the Mediterranean area (10). Patients who are carriers of the mutation are more susceptible to thrombophilia, especially at a younger age. Activated protein C resistance is responsible for 30% cases of thrombosis, whereas the presence of mutations increases the risk of thrombosis 3–7 times (11,12). In the healthy population the risk for the development of VTE is 1 per 1,000 per year. The risk in carriers of one polymorphic allele of FV Leiden is 4–8/1,000 and for the homozygotes 80/1,000 per year (13).
In 1996 Poort and his group have described the single nucleotide mutation in the gene of prothrombin that is associated with an increased risk for thrombosis. It is a single base exchange in which guanine replaces adenine at the position 20210 in the regulatory 3’of the gene that encodes this factor. The change in the genome results in an increased gene expression (14). In patients who are carriers of the mutated allele an increased activity of prothrombin in plasma was observed. Results of the study by Margaglione shows that the frequency of this mutation is higher in the patients with the thromboembolic disease when compared to the controls (8.01% compared to 2.29%, P < 0.001) and its presence increases the risk for thrombosis with OR (95% CI) = 3.88 (2.23–6.74) (15). The prevalence of heterozygotes in the population is 0.7–4.0%, being the most common in European population (16). According to the results of large Leiden Trombophilia Study (LETS), the frequency of FII G20210A mutation was higher in the group of patients with the thromboembolic disease when compared to the healthy population (6.2% vs. 2.3%, relative risk = 2.8) (17).
According to literature data, the relative risk of thrombosis is two times higher in patients with the prothrombin gene mutation, three times higher in patients with the mutation for FV Leiden and six times higher in patients who are carriers of both mutations, compared to patients who have the wild-type genotype for both genes. The incidence of venous thromboembolism is lower in prothrombin mutation carriers compared to FV mutation carriers (18).
Besides the above mentioned genetic factors, hyperhomocysteinaemia is also associated with a significantly higher risk of developing an early atherosclerosis and venous thromboembolism (19). Frost has described the single nucleotide polymorphism C677T in the coding region of the methylenetetrahydrofolate reductase (MTHFR) gene (20). Incidence of heterozygotes for this polymorphism is about 45% and the incidence of homozygotes is approximately 15% in the general population (21). In the carriers of polymorphic allele, the newly formed protein is thermolabile, and at 37 ºC its enzyme activity is reduced to 50%. Many studies have shown that carriers of both polymorphic alleles have moderately increased concentration of homocysteine. The exact impact on the occurrence of venous thrombosis has been unclear so far, but it is quite obvious that the presence of hyperhomocysteinemia increases the risk for thrombosis (22). In the Leiden Thrombophilia Study, homocysteine concentration above the 95th percentile significantly increased the risk for thrombosis with the OR (95% CI) = 2.5 (1.2–5.2).
The plasminogen activator inhibitor-1 (PAI-1) promoter 4G/5G insertion/deletion polymorphism is associated with changes in plasma concentration of PAI-1, being 25% higher in mutated allele carriers than in wild-type individuals. According to previous studies, the 4G allele represents an additional risk factor for the occurrence of deep venous thrombosis and myocardial infarction at a younger age in combination with other risk factors (23,24).
While reports on the prevalence of genetic risk factors for thrombophilia are numerous, there are only few reports on this in Croatian population (25,26). It has long been reported that prevalence of various genetic factors significantly differs across different regions within Europe, as well as on the global world level. We have therefore undertaken this study to examine the frequency of FV Leiden, FII G20210A, MTHFR C677T and PAI-1 4G/5G polymorphisms in Croatian patients with thromboembolic disease and to determine whether there is a difference in polymorphism frequency between patients with VTE and healthy subjects.
Materials and methods
Patients
This prospective study was conducted in the period of 2004–2005 at the Intensive care Unit of the Department of Internal Medicine, Sestre milosrdnice University Hospital. All patients who were treated for venous thromboembolic disease were consecutively included in the study.
For the purpose of comparison, a group of 106 healthy individuals, recruited at the primary health care giver, was also included in this study. The healthy individuals had no personal or family record of thromboembolic disease and were free of any systemic, cardiovascular, malignant and inflammatory disease at the time when they consented to enter the study.
In all patients the diagnosis of deep venous thrombosis was confirmed by leg duplex scan blood vessels ultrasound (ATL HDI-500, Solingen, Germany). The diagnosis of pulmonary embolism was confirmed according to Guidelines for the Management of Suspected Acute Pulmonary Embolism (27). Patients were treated and followed according to the standard protocol (28).
Demographic characteristics (age, gender) and known risk factors for the thromboembolic disease were collected for all participants of the study.
All cases and controls were fully informed about the study protocol by the main investigator and have consented to participate in the study by signing the written consent. The study was approved by the Ethics Committee of the hospital.
Methods
The DNA was isolated from EDTA anticoagulated whole blood (Vacutainer Becton Dickinson, Meylan Cedex, France) using the commercial QIAamp DNA Blood Mini Kit (250) (QIAGEN GmbH, Hilden, Germany). The FV Leiden, Factor II G20210A, MTHFR C677T and PAI-1 4G/5G polymorphisms were genotyped by real time PCR and melting curve analysis using Light Cycler 1.2 (Roche Diagnostics, Mannheim, Germany).
Statistical analysis
The data were presented as counts and percentages. Differences between groups were tested with Chi-square test. The Fischer exact test was used for those groups where relative frequencies were low. Age differences between groups were assessed using t-test. Statistical significance was set at 0.05. All groups were tested for Hardy-Weinberg equilibrium. Statistical analysis was performed by using the MedCalc R 10.1.1.0 statistical software (Franck Schoonjans, Mariakerke, Belgium).
Results
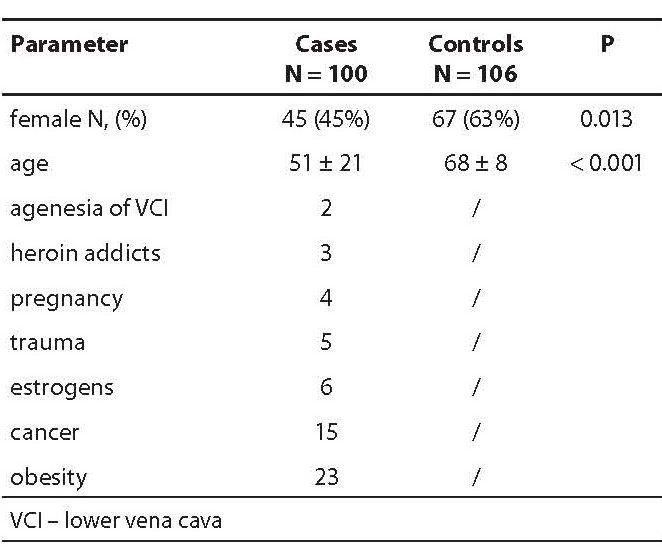
This study included 100 patients with the venous thromboembolic disease and 106 healthy individuals. Demographic characteristics are summarized in Table 1.
Table 1. Demographic characteristics of cases and controls.
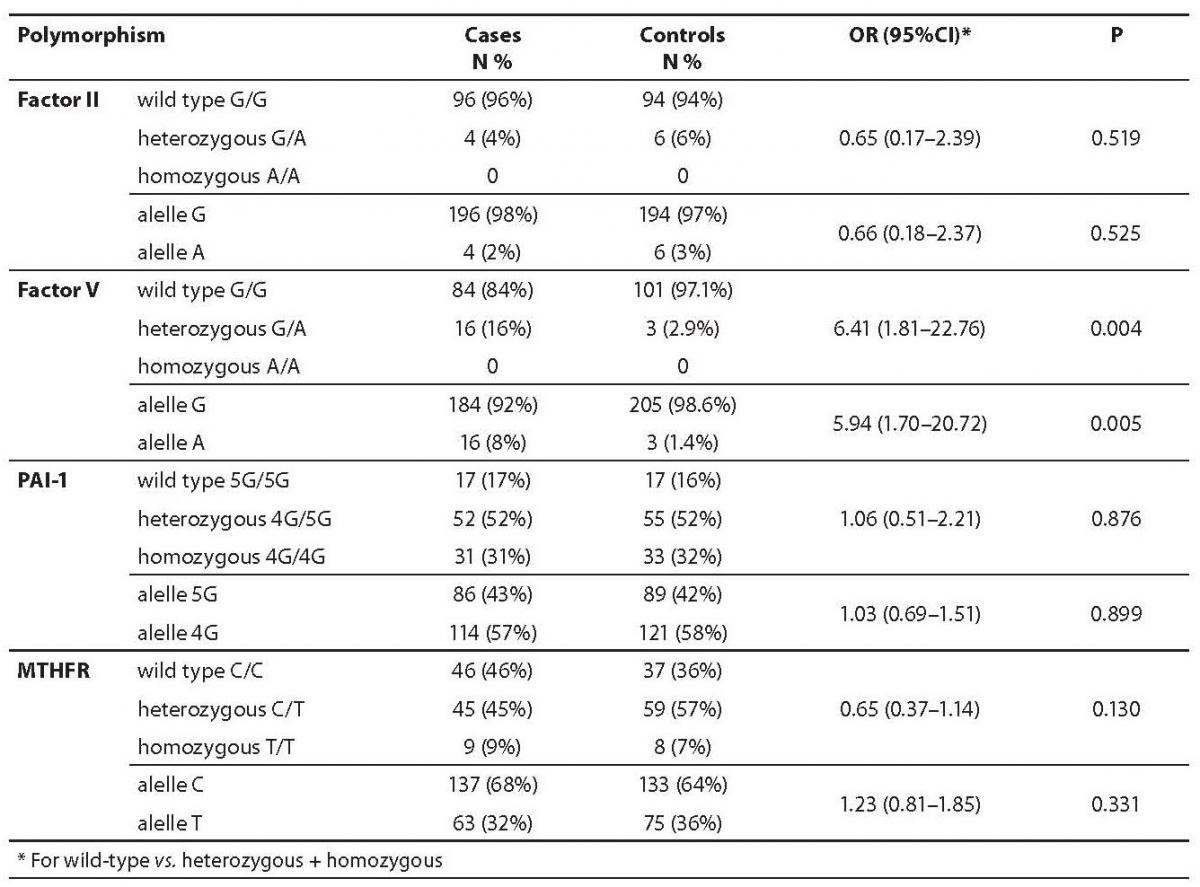
Out of four tested polymorphisms, only the FV Leiden polymorphism showed to be significantly associated with venous thromboembolic disease with an odds ratio OR (95% CI) = 6.41 (1.81–22.76); P = 0.004. When patients with other known risk factors were excluded from the patient group, the risk for the occurrence of thromboembolic disease due to the isolated FV Leiden genetic polymorphism (N = 44) was even higher with OR (95% CI) = 9.81 (2.69–35.79); P < 0.001.
Allele and genotype frequencies of F II G20210A, MTHFR C677T and PAI-1 4G/5G polymorphisms did not differ significantly between cases and controls. Allele and genotype frequencies are presented in Table 2.
Table 2. Allele and genotype frequencies in patients and controls.
Discussion
We have investigated the frequency of FV Leiden, FII, MTHFR, and PAI-1 polymorphisms and their association with VTE in the Croatian population. The limitation of our study was the small number of patients in the subgroups.
Venous thromboembolic disease is a hereditary common disease of the Caucasian population that can be caused by a number of genetic and environmental risk factors that enhance the procoagulation tendency. It is important to emphasize that the presence of polymorphic allele only by itself is not sufficient for the occurrence of thrombosis. All studies conform to the multifactorial etiology of the disease. The risk of the thromboembolic disease increases in proportion to the number of risk factors (29).
Factor V Leiden, which renders FV resistant to activated protein C (APC) degradation, is the most common inherited risk factor in Caucasians, with an average prevalence in healthy population of about 4.4% (2–15%), about 18% in patients with the thromboembolic disease and about 40% in families with history of thrombophilia (30,31). The evolutionary origin of the mutation was found in the central part of Europe in the Neolithic Age. The prevalence increases from West to East Europe and decreases from south to north of Europe. Factor V Leiden is rarely found in African, Australian and South Asian population, while in Asia Minor its frequency is only 0.7%, which partly explains the fact that the incidence of thrombosis in these countries is low. It is also very rare in French population Basques (10,32). In our study, the frequency of the heterozygous for FV Leiden polymorphism in the control healthy subjects is 2.9%, while it is higher in the group of patients with thromboembolic disease (16%). The prevalence of factor V Leiden and prothrombin G20210A has already been described for Croatian population in the study by Cohen and collaborators in 2001 (25). A slightly higher frequency of mutations for factor V and prothrombin G20210A (21%, 8%) in the 160 Croatian patients with the VTE was observed. Although the prevalence of mutations among our patients is lower, our results concur with previously reported prevalence for Caucausian populations.
The second most important inherited prothrombotic risk factor, FII G20210A polymorphism is present in Caucasian population with the frequency of 0.7 to 4%, with an average about 2%. The prevalence in the Mediterranean area ranges around 3.0% (95% CI = 2.3–3.7%), while in northern Europe the frequency of mutations in the population is two times smaller (1.7% (95% CI = 1.3–2.2%)). The greatest frequency of polymorphism in the world is found in Mexican population, where the prevalence is extremely high (13.5%) (16,33). The prevalence of this mutation in the VTE patients is 8%, and even higher prevalence (18%) is found in selected families with thrombosis (14). As for Factor V, there were no homozygous patients for FII G20210A in our study. In our investigated groups there were 4% VTE patients and 6% healthy controls heterozygous for this polymorphism. The statistical analysis has shown no significant difference in the prevalence of polymorphisms between groups which does not correspond to literature data. The values on the frequency of FII G20210A polymorphism in the control group are consistent with the data published in other studies However, it is important to emphasize that a small number of respondents included in our study is not sufficient for generalizing the data on the entire population, due to the small sample size and limited power of the study. That partly explains the lower frequency of the factor II polymorphism among patients.
The polymorphic allele frequency of PAI-1 varies among races and ethnic groups. The presence of the 4G allele is increased in the white population in relation to the Africans and is associated with the thrombotic disease in combination with other thrombophilia defects (34). Based on the published data, the prevalence of the 4G allele carriers in the Caucasian population is about 76%, 50.5% of which are heterozygotes (4G/5G) and 26.3% homozygotes (4G/4G) (35). The prevalence of the polymorphism in our study (52% heterozygous and 17% homozygous) was identical in both studied groups and is in agreement with the literature data (36).
The prevalence of the T allele also varies among races and ethnic groups. It is more common in Caucasians and Asians (0.30) compared to African Americans (0.11). The studies have shown certain differences among the European populations. The frequency of heterozygotes (C/T) is the largest in Italy 44%, as opposed to Norway, where it is lower (28%). Meta analysis of studies among European populations has shown that the frequency of homozygotes (T/T) ranges from 5–15% (21).
A study by Lovričević et al., published in 2004, conducted on 228 Croatian volunteers has found 9.21% homozygotes (T/T), 44.74% heterozygotes (C/T) for the mutation and 46.05% carriers of the wild type (C/C). These results are consistent with the prevalence of mutations in European populations (26). In our study the statistical analysis showed no significant difference in the incidence of mutations between the groups. The frequency of 9% homozygous and 45% heterozygous cases among patients is consistent with the data from the literature.
The frequency distribution of examined polymorphisms (FV Leiden, MTHFR, PAI-1) is in accordance with the findings already reported in other Caucasian populations. Only a slightly lower frequency of factor II G20210A among patients deviates fromthose factors results. FV Leiden and factor II G20210A have been described as the most important inherited prothrombotic risk factors in recent literature (11–15). MTHFR and PAI-1 contribute to the risk in combination with other factors (35,37). In our group of patients only FV Leiden corresponded with an increased prothrombotic disease risk OR (95% CI) = 6.41 (1.81–22.76), especially when patients with an environmental risk factor were excluded from the study OR (95% CI) = 9.81 (2.69–35.79). FII G20210, MTHFR and PAI-1 polymorphisms were not associated with venous thromboembolism in our study. A small sample size and low frequency of the factor II heterozygotes among patients may partially explain the lack of association for the factor II. These results give us some new information on thrombosis related genetic polymorphism in Croatian population. Given the small number of patients included by this study, more informative results could be obtained by a broader study with a larger sample.
Conclusion
Based on our results, herein we conclude that only Factor V Leiden was significantly associated with thromboembolic disease in our patients. The analysis showed that the presence of other three studied polymorphisms (Factor II G20210A, PAI-1 5G/4G and MTHFR C677T) were not associated with venous thromboembolism in our study.