Introduction
The human immune response is a highly complex and delicate balance between pro- and anti-inflammatory mechanisms and involves cells as well as cytokines. When the immune system is activated, for example by bacterial infection, the immune response is normally strictly regulated and the pro- and anti-inflammatory phases are balanced and synchronized. In systemic inflammatory response syndrome (SIRS) the immune system is over-stimulated and the pro-inflammatory response precedes the anti-inflammatory reaction: the normal balance is disturbed and out of phase. The excess of pro-inflammatory cytokines causes excessive activation of leukocytes, release of lytic enzymes and toxic radicals and endothelial damage, which results in increased vascular permeability, circulatory disturbances and eventually organ failure. The excessive anti-inflammatory phase causes immune suppression, which makes the patient more prone to secondary infections (1).
SIRS is not necessarily caused by infection as other events like major surgery, severe trauma or burns can also induce SIRS. When a patient with SIRS acquires a bacterial infection, he may develop sepsis, which can further progress to severe sepsis, septic shock and finally death (2,3). Despite advances in antibiotics treatment, the mortality of sepsis is still high; some studies report up to 50% of patients dying of sepsis (4,5). A major reason for this high mortality is that treatment is often started at a time where irreversible damage is already inflicted. Once sepsis is clinically suspected, early commencement of antibiotic therapy increases the chance of survival (6).
The golden standard for diagnosing sepsis is still blood culture (7,8). A serious disadvantage of this test is that it can take up to 2 days before the final result is available and during this period, the condition of a septic patient can rapidly deteriorate. Therefore, it is common practice to start therapy with broad-spectrum antibiotics before the results of blood culture are known. However, administration of antibiotics to patients who have no bacterial infection is not only unnecessary, but is expensive and can contribute to developing bacterial resistance to antibiotics, too. Therefore, clinicians are in need of biomarkers that can reliably detect sepsis or its associated infection in an early stage or exclude infection so that timely decisions on starting or terminating antibiotic treatment can be made (7,8).
Neutrophil CD64 as a biomarker
Expression of the CD64 antigen on neutrophils has been under investigation for some years as a biomarker of infection and sepsis. It has several characteristics that make is well suited for clinical application: on resting neutrophils CD64 expression is low and after activation it is significantly upregulated within few hours. Once the activation stimulus disappears, CD64 expression returns to its basal level in few days. Moreover, CD64 is relatively stable after blood collection and the assay is straightforward and requires only small sample volume. Last but not least, CD64 expression represents a physiological process which plays a key role in the innate immune response: neutrophils acting as phagocytes.
The CD64 antigen is the high affinity receptor for the Fcγ part of the IgG heavy chain and can bind monomeric IgG1 and IgG3 as well as aggregated IgG (9). Phagocytosis of bacteria and other microorganisms is mediated by this FcγRI receptor. In contrast to monocytes where CD64 antigen is constitutively expressed, resting neutrophils have very low levels of CD64 antigen on their membrane, approximately 1000 molecules per cell (10). CD64 expression is increased upon activation of neutrophils by pro-inflammatory cytokines within 4-6 hours and can reach more than 10-fold higher levels than in resting conditions, allowing good discrimination between resting and activated neutrophils (11,12).
Diagnostic performance in adults with sepsis
In the last few years various investigators have focused their research on the clinical utility of neutrophil CD64 as a marker for sepsis or systemic infection (Table 1). Davis was the first who reported a study in which CD64 was measured in patients who were later determined to have had sepsis (13). As this study was retrospective and samples selection was performed in the hematology laboratory, it should be best regarded as a “proof of principle” investigation. Anyway, it demonstrated the diagnostic potential of CD64 and also showed that neutrophil CD64 performed better than all other laboratory tests that were then in use. A subsequent study by the same group prospectively included patients presenting at the emergency department. The results confirmed those of their previous study: CD64 had the highest sensitivity and specificity in detecting systemic infection or sepsis (14). Remarkably, the cut-off level used for neutrophil CD64 was considerably lower than in the first study; unfortunately an explanation was not provided (13,14). Livaditi and coworkers reported the first study that enrolled critically ill patients from an intensive care unit (ICU), which represents the clinical situation in which sepsis biomarkers likely have the most relevant application. These authors found that serum interleukin-6 (IL-6) and IL-8 as well as neutrophil CD64 best evaluated the severity of sepsis in an early stage, whereas CD64 and IL-8 could also predict mortality (15). A larger study involving adult sepsis patients was published by Cardelli et al (16). They included 112 ICU patients who were clinically suspected of having sepsis; in 52 of these patients sepsis was proven by positive blood culture. Neutrophil CD64 was able to distinguish these patients from the ones in whom sepsis could not be proven with very high sensitivity and specificity. Moreover, CD64 appeared to be more specific than procalcitonin (16). A similar study, albeit in a much lower number of patients, was undertaken by Danikas and colleagues, who showed that high CD64 expression on neutrophils was favorably correlated with survival (17). Another small study in patients suspected of sepsis thus far only appeared as an abstract with limited details; also here high sensitivity and specificity for identifying patients with positive blood culture was reported (18).
Further, a recent report by Hsu et al showed that in patients in a respiratory ICU neutrophil CD64 was better than procalcitonin for distinguishing SIRS from severe sepsis and septic shock (19). In addition, CD64 was found to be associated with mortality in this study. Very recently Gámez-Díaz et al. published the results of the largest study ever (20). They investigated emergency department patients with suspected infection, fever, delirium or acute hypotension of unclear origin. Of the 631 patients included, 416 (66%) were deemed to have sepsis. The sensitivity of neutrophil CD64 for a diagnosis of sepsis was 66% and the specificity 65% (20).
Further, a recent report by Hsu et al showed that in patients in a respiratory ICU neutrophil CD64 was better than procalcitonin for distinguishing SIRS from severe sepsis and septic shock (19). In addition, CD64 was found to be associated with mortality in this study. Very recently Gámez-Díaz et al. published the results of the largest study ever (20). They investigated emergency department patients with suspected infection, fever, delirium or acute hypotension of unclear origin. Of the 631 patients included, 416 (66%) were deemed to have sepsis. The sensitivity of neutrophil CD64 for a diagnosis of sepsis was 66% and the specificity 65% (20).
Table 1. Summary of studies on the diagnostic performance of neutrophil CD64 in adult patients with sepsis.
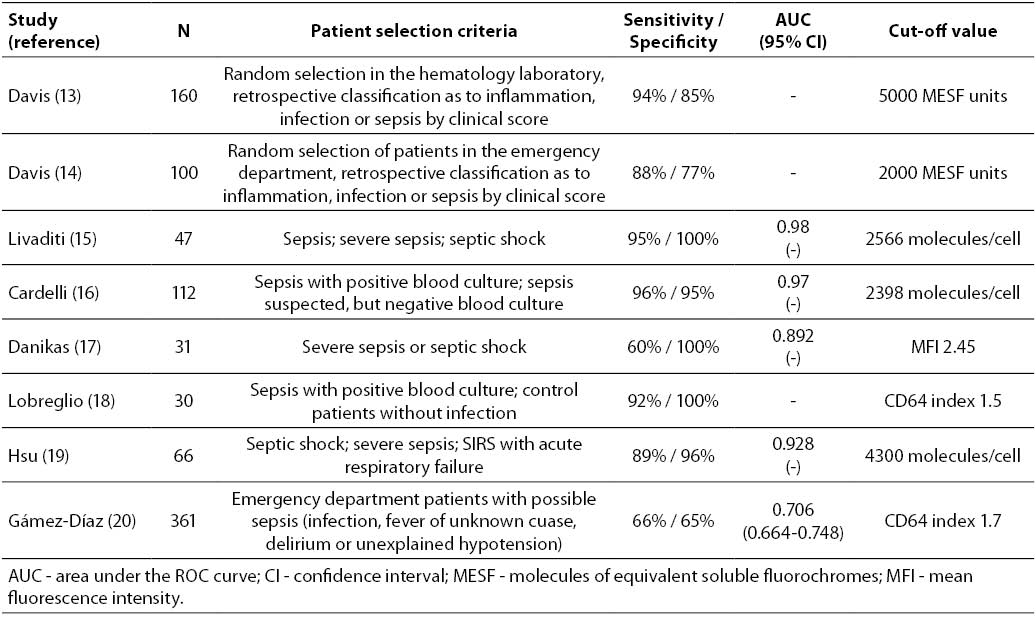
A critical overview of almost all the above studies is provided in two recent review papers (21,22). Unfortunately, most of the studies have been performed on relatively small patients groups and have serious methodological shortcomings (22). Nonetheless, the results are generally well in agreement. The pooled sensitivity of CD64 for detecting infection or sepsis was reported as 79% and the specificity 91% (22). However, the calculations in this meta-analysis were performed using studies with highly variable design: both adults and neonates were included and patients with sepsis, systemic infections and local infections were mixed, which is not representative of neutrophil CD64 as a sepsis biomarker. When considering studies on septic adult patients only, the overall sensitivity would be 88.3% (95% confidence interval 78.1-94.1%) while the specificity would amount to 87.6% (71.8-95.2%) (Table 1). Combining these studies has its limitations, though. The individual studies had highly different designs, the inclusion criteria were not always similar, they generally used small numbers of patients and there was substantial variation in analytical methodology as well as in definition of the cut-off value (Table 1). Taken together, there is evidently a need for much larger, multicenter studies with uniform inclusion criteria and standardized analytical methods in order to fully appreciate the clinical utility of neutrophil CD64 as a sepsis marker in an ICU setting.
Diagnostic performance in neonates and children with sepsis
Neonatal sepsis is different from adult sepsis in several respects and therefore a separate discussion is warranted. The clinical signs and symptoms often are more subtle and non-specific than in adults, a clinical score system has no clear advantage and traditional laboratory tests have poor diagnostic performance (23,24). Therefore, neutrophil CD64 would be a candidate sepsis biomarker also in neonates and children. However, healthy neonates reportedly have higher CD64 expression on their neutrophils than adults (25,26), which might influence the diagnostic power of the test.
Table 2 summarizes the current literature on neutrophil CD64 as a biomarker for neonatal and childhood sepsis. Layseca-Espinosa et al. showed that neutrophil CD64 was a highly specific indicator of neonatal sepsis, albeit with low sensitivity (27). These authors used the percentage of CD64-positive cells as a criterion; however, it has been shown that CD64 fluorescence intensity, either as mean fluorescence index (MFI) or as an index relative to standard beads, is a better discriminator than percentage CD64-positive neutrophils (28,29). Ng and colleagues demonstrated the utility of CD64 as a biomarker of late-onset infection in preterm, very low birthweight infants: both at the first clinical suspicion of sepsis as well as 24 hours later, the diagnostic performance of neutrophil CD64 was much better than all other markers investigated (30). The combination of neutrophil CD64 expression with either serum C-reactive protein or IL-6 even enhanced the sensitivity to 100%, meaning that these markers together can be used to exclude infection (30). Some years later the same group published a very similar study, but now on early-onset infection in term infants; they enrolled the largest number of patients reported up to now. This study confirmed the very high sensitivity of neutrophil CD64, but in contrast to their previous study addition of CRP improved the diagnostic power of CD64 only marginally (31). A smaller study in critically ill neonates and infants by Groselj-Grenc used the standardized CD64 index for the first time and demonstrated its superiority over all other infection markers (29). In a follow-up study the same authors presented evidence that neutrophil CD64 was the best individual marker for bacterial sepsis in children, whereas the test performed somewhat less in neonates (32). However, both patient groups were of limited size and might actually not warrant this conclusion. Bhandari et al. conducted the third-largest study in neonates with suspected sepsis and also these authors found that neutrophil CD64 index had the best diagnostic performance for culture-positive sepsis compared with all traditional hematologic assays (33). In the study by Dilli et al., performed on over 100 patients in a neonatal ICU, the neutrophil CD64 index again was found to be the test with the highest sensitivity, with no difference between neutrophil CD64 index and MFI (34). Combination of CD64 index with CRP and IL-6 increased the sensitivity and the negative predictive value to 100%, allowing reliable exclusion of infection. Slightly lower diagnostic performance was reported by Zeitoun and coworkers, also when the CD64 index was combined with serum IL-10 (35). Recently, Lam et al. demonstrated in a large-scale study that neutrophil CD64 was useful in neonates suspected of abdominal infection and sepsis, in particular in combination with conventional X-ray imaging for excluding an infectious cause of disease (36).
Table 2. Summary of studies on the diagnostic performance of neutrophil CD64 in neonates, infants and children with sepsis.
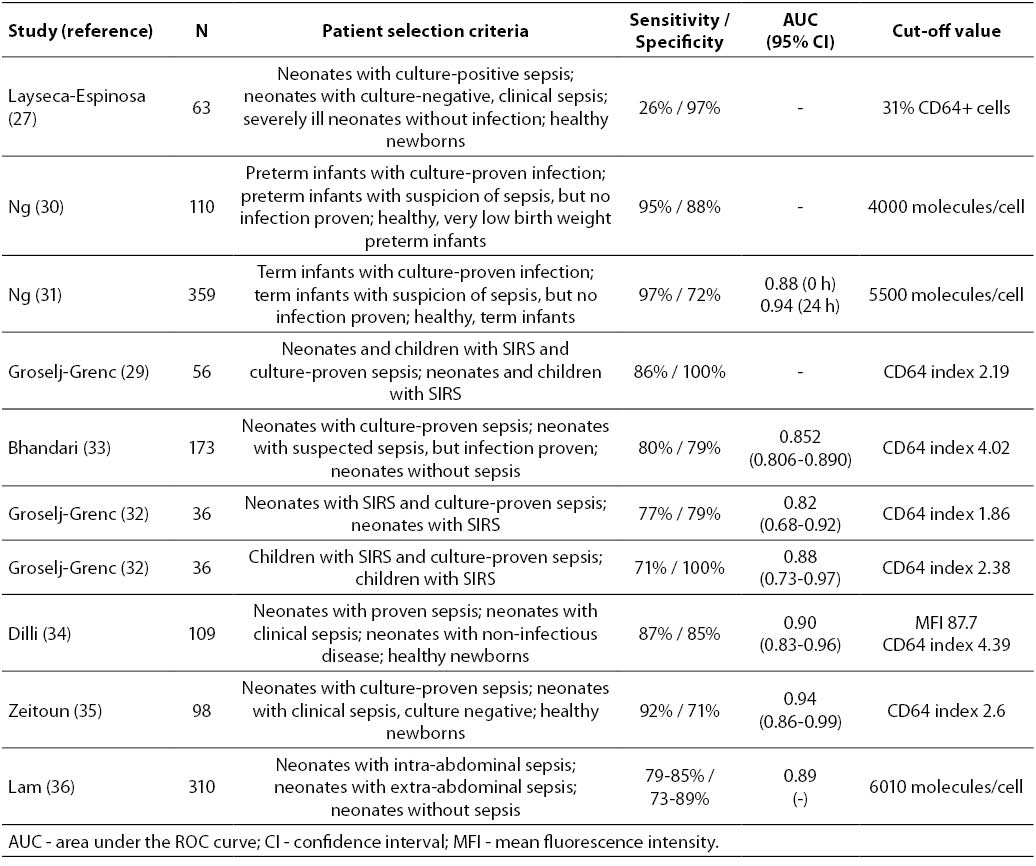
Overall, these nine studies in neonates and children give a reasonably consistent impression of the diagnostic performance of neutrophil CD64 in sepsis and severe infection. The composite sensitivity (83.4%; 95% CI = 70.0-91.5%) and specificity (86.2%; 95% CI = 75.2-92.7%) show that CD64 represents one of the most sensitive biomarkers of pediatric sepsis currently available for clinical use.
Until recently it seemed that neutrophil CD64 had higher sensitivity and specificity in adults with sepsis than in neonates and children. However, the most recent paper (20) changed the situation. The summary ROC curves of adults and neonates and children do no longer show statistical differences and therefore can reliably be combined. The overall summary ROC curve demonstrates that neutrophil CD64 can detect sepsis with a sensitivity of 85.7% (95% CI = 77.5-91.2%) and specificity of 87.4% (95% CI = 79.3-92.6%), as shown in Figure 1. The positive likelihood ratio is 6.79 (95% CI = 4.02-11.47) and the negative likelihood ratio 0.16 (95% CI = 0.10-0.26).
Figure 1. Summary ROC curve of 17 studies reporting on the diagnostic performance of neutrophil CD64 as a sepsis biomarker. Each study is represented by a square, the size of which is proportional to the number of patients included. The black dot is the composite sensitivity and specificity; the area around it represents the 95% confidence range.
Marker of disease severity
Neutrophil CD64 expression is not only useful for the diagnosis of systemic infection and sepsis, but several authors have also reported its value as an indicator of sepsis severity: patients with septic shock generally show the highest CD64 values, higher than in severe sepsis and much higher than in sepsis and SIRS (12,15,19,37). The latter authors also demonstrated that patients receiving adequate antibiotic therapy had a quick decrease of their CD64 index, in parallel with an improvement in their clinical condition (37). It is not only in sepsis that CD64 is a good indicator of disease severity; the same finding has been reported in local infections, too (38).
Prognostic information
According to several authors, neutrophil CD64 contains also prognostic information as to survival. However, the available data are highly contradictory. Several publications reported that survival could be predicted by a low CD64 expression (12,15,19,39,40), whereas others indicated that high CD64 would be an indicator of favorable prognosis (17,41). Most likely the small patient groups and the design of the studies explain these conflicting findings.
Diagnostic performance in other infective and inflammatory diseases
Apart from systemic infection and sepsis, there is a wide variety of other disease states in which the diagnostic utility of neutrophil CD64 has been suggested. One of the most useful applications is probably the ability of neutrophil CD64 to distinguish between bacterial infection and acute flares in rheumatoid arthritis and other autoimmune disorders (42-47). Further, CD64 has been found useful as a marker of postoperative infection in patients undergoing musculoskeletal (38), cardiac (48) or vascular surgery (49). CD64 index was a valuable tool in inflammatory bowel disease, too (50). A recent review indicated that neutrophil CD64 is not only increased in bacterial infection, but also in viral infection, depending on the type of virus (26). Finally, CD64 has successfully been used in familial Mediterranean fever (51) and as a rejection marker in transplant patients (52).
Analytical aspects of neutrophil CD64 assay
Flow cytometry is the method of choice for determining neutrophil CD64. In the early years authors used density gradient centrifugation for isolating neutrophils followed by indirect immunofluorescence for detecting CD64 expression. Nowadays, virtually all investigators use direct immunofluorescence in whole blood using a lyse-no-wash method (13,29). The intra-laboratory imprecision seems to be low with coefficient of variation 3-6% and < 12%, respectively (53,54). Data on the inter-laboratory variation have not been reported. The assay can conveniently be performed in a small volume of EDTA-anticoagulated blood and the CD64 antigen is stable for 36 or 72 hours at room temperature (13,50).
Like with most flow cytometric assays, the determination of neutrophil CD64 lacks standardization. As shown in Tables 1 and 2, various methods are in use for expressing CD64 on neutrophils: percentage of CD64-positive cells, mean or median fluorescence intensity (MFI) and as an index relative to standardized beads. The latter method is available as a commercial kit (Trillium Diagnostics, Brewer, ME, USA). It comes in two formats: one for use on flow cytometers (32,35,37,55) and one for the CELL-DYN Sapphire hematology analyzer,
which allows practical full automation and does not require flow cytometry expertise (18,41,54,56). Both kit methods use FITC-labeled CD64 and PE-labeled CD163 monoclonal antibodies and contain calibrated fluorescent beads for standardization. Lymphocytes and monocytes are used as negative and positive internal control, respectively. The assay requires 50 µL of blood and can be completed within 1 hour on a standard flow cytometer and within 20 minutes on the Sapphire analyzer. Thanks to the calibrated beads, the kit method has the potential of inter-laboratory comparability of
results, although data have not yet been published.
which allows practical full automation and does not require flow cytometry expertise (18,41,54,56). Both kit methods use FITC-labeled CD64 and PE-labeled CD163 monoclonal antibodies and contain calibrated fluorescent beads for standardization. Lymphocytes and monocytes are used as negative and positive internal control, respectively. The assay requires 50 µL of blood and can be completed within 1 hour on a standard flow cytometer and within 20 minutes on the Sapphire analyzer. Thanks to the calibrated beads, the kit method has the potential of inter-laboratory comparability of
results, although data have not yet been published.
Critical assessment of the literature
The general picture that arises when reading the available literature is that neutrophil CD64 seems to be a highly sensitive and reasonably specific biomarker for sepsis and other infections. However, there are several factors that should nuance these positive reports. The two most important have already been mentioned above: nearly all studies included relatively small patient numbers and the methodological quality of reported studies is mediocre (22). In addition, there is an enormous variation in criteria for selecting patients, differences in the definition of sepsis as well as poorly standardized analytical methodology. Sometimes, healthy subjects are used as a control group, which does not represent the conditions in which a sepsis biomarker is clinically used and moreover, this practice can easily overestimate the power of a diagnostic test.
This all does not mean that we should disregard these studies. They present a highly promising and strong indication, but not sufficiently solid scientific evidence that neutrophil CD64 expression is a biomarker for sepsis that can be recommended for routine use. This needs to be confirmed by large-scale, prospective, multicenter, preferably case-control studies of good methodological quality. The definition of sepsis should be in accordance with widely accepted criteria (2,3), blood cultures should be performed as the reference standard, patients in whom sepsis was clinically suspected but could not be objectively proven should be used rather than healthy controls for calculating sensitivity and specificity for sepsis patients, the analytical method for CD64 should be standardized and calibrated using beads. In addition, disease severity should be scored using well accepted systems and the clinical follow-up should be long enough to document sepsis-related mortality. Furthermore it would be interesting to study neutrophil CD64 as a tool for monitoring therapy, like is currently being done for procalcitonin.
Conclusions
Despite the poor methodological quality of the available literature, it is evident that neutrophil CD64 is a very promising sepsis biomarker, undoubtedly much better than traditional hematologic parameters and CRP and probably also better than procalcitonin (57). Neutrophil CD64 seems to perform equally well in adults and in neonates and infants. The CD64 assay is relatively simple and can easily be implemented in practice. However, validation in large multicenter studies is required before neutrophil CD64 can be recommended as a sepsis biomarker for routine use in ICU patients.
Acknowledgements
The author is indebted to Fabian Röthleithner for his expert statistical advice.